- Department of Plastic Surgery
Department of Plastic Surgery » - Center for Reconstructive Plastic Surgery
Center for Reconstructive Plastic Surgery »
- Articles by our doctors
Articles by our doctors »
- Autologous fat grafting in reconstructive breast surgery
Scientific and practical journal “Povolzhsky Oncological Bulletin”, 2015. No. 3, pp. 4-8
The author of the article is Semyon Igorevich Fedosov, reconstructive plastic surgeon at the RAMI clinic.
Introduction
Lipofilling (autotransplantation of fat) is the correction of body contours by transplanting autogenous adipose tissue from the donor area to the recipient area using injections.
The use of autogenous adipose tissue is possible for any conditions that are characterized by atrophy or defect of subcutaneous adipose tissue, as well as if the patient wishes to change the contour of a particular part of the body.
There is no need to talk about the advantages of your own tissue over synthetic injectable materials or implants. The use of adipose tissue in reconstructive plastic surgery has been known for a long time; in 1883, Neuber first proposed the idea of transplanting the patient’s own adipose tissue to replace the volume of subcutaneous soft tissue. In 1889, Van Der Meulen used the greater omentum, removed during surgical treatment of a diaphragmatic hernia, as a fat graft. T. Czerny in 1895, performed breast augmentation through lipoma transplantation. Lexer in 1920 performed breast augmentation using fat pads as a filler. Erich Lexer also owns a two-volume treatise, Die Freien Transplantationen (free transplantation), published in 1919, containing almost 300 pages on the technique of fat tissue transplantation. However, by this time the disadvantages of fat tissue grafting had already been noted. Thus, F. Verderame noted that the transplanted fat has a tendency to be reabsorbed, and therefore recommended transplantation with hypercorrection. And in 1925, Davis and Traut published data on methods for increasing the effectiveness of fat tissue transplantation. In 1929, O. Loewe proposed including dermis in the fat graft, which, according to the author, not only gave it density, but also provided better vascularization. By the beginning of the 40s of last year, the number of works devoted to the problem under study increased. Errors and complications were analyzed, new methods of using fat were proposed, and a study was carried out on the speed and volume of fat loss after transplantation. Bames in 1953 reported on the possibility of breast augmentation using the patient's own adipose tissue as a filler. Of course, the result of these “experimental” operations was unsatisfactory, because At that time, there was no modern understanding of the anatomical and physiological properties of adipose tissue. The first publication reflecting retrospective results of the use of adipose tissue in plastic surgery of the mammary glands dates back to 1987 and is devoted to the “microinjection technique of mammary gland augmentation using lipoaspirate obtained after liposuction” (Bircoll et al). In 1988, the American Society of Plastic Surgeons published an article, “Banned the Procedure,” which detailed the “dark side” of autologous fat grafting and described the technique as “flawed.”
However, the accumulation of experience and knowledge in the field of using adipose tissue as a plastic material and the definition of the lipografting procedure from the perspective of transplantology made it possible to formulate a modern and effective concept of using a fat graft.
Transplantation of one's own adipose tissue, as a separate technique for breast reconstruction, was described in 2000 in the article “Reconstruction after mastectomy and lumpectomy; Delay/ Rigotti.” However, in the same year, a work was published: “the method of fat tissue transplantation is good as an addition to breast reconstruction, unsatisfactory as a method of primary reconstruction...” (American Society of Plastic Surgeons), which describes in detail and justifiably a number of unsolved problems that limit the use of this techniques as a mono-tool for reconstructive surgery of the mammary glands.
Currently, research is ongoing into the dependence of the survival rate of adipocytes on the technique and area of fat harvesting. A search is underway for a universal donor area. Morphological studies of the transplanted adipose tissue are carried out and the degree of its resorption is determined. The process of fat graft vascularization and its effect on the survival rate of transplanted adipocytes is being studied. Methods for pre-injection treatment of adipose tissue are being developed in order to increase its viability. Despite great achievements in these areas, many issues still remain unresolved.
So, taking into account all of the above, the question naturally arises: “Has the role and consistent method of fat tissue transplantation been determined?” Is it possible to widely and actively use this technique? All of the above suggests that it is necessary to clearly formulate the indications, contraindications and target audience of patients for whom the lipofilling method is not only possible, but also safe.
Based on the information received, our center began active work to introduce this technique into clinical practice.
Rehabilitation period
Immediately after lipomodeling of the buttocks, the patient is put on special shaping underwear and wears it during the day for several weeks. The patient is discharged the next day after surgery. In the first few days after surgery, you may experience a feeling of tension in the skin at the operation site due to postoperative swelling. For 2-3 days, moderate pain is felt in the area of the operation, which is calmed down by taking medications. The swelling subsides within a week. Within a week you can return to normal life and go to work, avoiding heavy loads.
Materials and methods
From June 2014 to July 2020, we performed 54 operations aimed at correcting the shape and volume of the mammary glands through fat tissue transplantation. All patients underwent careful selection and all had clear indications for the specified surgical treatment. Lipografting was not used in immunosuppressed patients or those scheduled for radiation therapy. In all cases, lipografting was used as an additional technique to the main reconstructive plastic surgery.
The main goals of using lipografting as an additional technique were: 1) increasing the projection; 2) filling the upper slope; 3) restoration of symmetry; 4) adding volume to the mammary glands after reconstructive operations using full-thickness complex autografts (flaps).
The main way to achieve these goals was to solve the following problems.
1. Obtain a sufficient volume of lipoaspirate. 2. Correlate the volume of lipoaspirate with the reserve capacity of the recipient zone. 3. Select the introduction layer. 4. Determine the frequency of operations.
Based on the principles of transplantology, the following stages of lipografting can be determined:
1) Determination of the zone of interest (recipient zone);
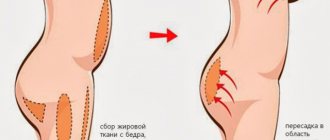
2) Selection of donor area. Preference is given to areas with a sufficient amount of fat: paraumbilical area, abdominal flanks, inner thighs, riding breeches, back, shoulders.
3) Anesthesia. Depending on the volume of fat taken and the number of donor areas, we use local anesthesia with intravenous potentiation or ETN. To collect fat, a tumescent technique is used: Sol. Lidocaini 10%-1ml+ Sol. NaCl 0.9%-400ml+ Sol. Adrenalini 0.5 ml. To prevent flooding of adipocytes, we abandoned the use of glucose and bicarbonate in the solution;
4) Fat removal. To obtain lipoaspirate with the maximum number of living adipocytes and minimize the content of blood in the lipoaspirate, we use: delicate cannulas, minimal vacuum (up to 0.6 bar), minimal aggression in the donor area;
5) Preparation for introduction. After taking the fat, the latter is centrifuged for 1.5 minutes at 1300 rpm; This ensures minimal contact of lipoaspirate with air, minimal transfer from system to system;
6) Introduction of fat. To inject fat, we use the micro-grafts technique, layer-by-layer retrograde injection without resistance. Hypercorrection is unacceptable, because The greater the volume of fat, the higher the risk of liponecrosis. At the introduction stage, strict adherence to the FTF (fat to fat) and FTM (fat to muscle) principles. To determine the permissible volume of transplanted fat into the recipient area, we are guided by the concept of “recipient capacity”; the amount of transplanted fat in one horizontal layer is limited by the capacity of 2 mm channels and the need to maintain no less distance between them, so as not to compromise the vascularization of the recipient bed. The boundaries of the injection zone can be expanded if lipofilling is carried out not in one, but in two or more tiers. You just need to remember that the vertical distance between the layers should be sufficient to maintain the same vascularized layer of recipient tissue between them;
7) Volume distribution.
All stages of the operation are aimed at improving the survival of fat.
In the postoperative period, bandages were applied to the puncture sites and antibiotic therapy was prescribed for two days. In this case, cold, pressure and massage of the recipient area were completely excluded.
Example #1:
Patient O., 33 years old. Diagnosis: cancer of the right breast, condition after complex treatment in 2012. BRCA mutation. Condition after bilateral subcutaneous mastectomy with simultaneous reconstruction with implants. Ripping in the area of the upper slope of the right breast.
Rice. 1 (a,b)
Example #2:
Patient X. 40 years old. Diagnosis: cancer of the left breast. Condition after complex treatment in 2013. Condition after subcutaneous mastectomy on the left with simultaneous reconstruction with an implant in combination with TDL, prophylactic subcutaneous mastectomy on the right with simultaneous reconstruction with an implant dated July 26, 2013. Deficiency of the upper slope of the mammary glands, cicatricial deformation of the lower slope of the right mammary gland.
Rice. 2 (a,b)
Depending on the clinical case, patients underwent one to three lipografting sessions. It should be noted that over the eleven-month follow-up period, the loss of adipose tissue in the recipient area ranged from 0 to 30%.
Limitations, benefits and frequently asked questions about breast fat grafting
Autotransplantation of fat is currently one of the most discussed topics in modern plastic surgery. Many patients are attracted not only by the advanced fat transfer techniques and impressive results, but also by the opportunity to use their own fat to shape their breasts. A procedure known as breast fat grafting (or breast lipoaugmentation) uses fat to increase volume. Thanks to this, the technology allows the surgeon to exercise some “flexibility” in giving the breast its final shape, since with implants the ability to form the volume of the mammary glands is somewhat limited.
Limitations in breast lipofilling
Even the most advanced fat grafting techniques have some limitations. The most important of them is that breast enlargement can only be increased by a certain volume in one operation. Typically, the maximum possible breast augmentation during one operation is limited to approximately 250 cm3, which is slightly larger than one size. The main reason for this transplantation rule is due to the limited space of the recipient bed.
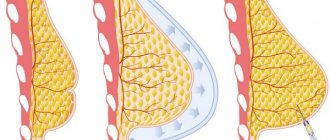
For safety reasons, injecting fat into the breast itself should be avoided. Fat can be safely transferred into the pectoral muscle, under the skin (subcutaneous) and into the so-called subglandular space. If done correctly, lipoautotransplantation of fat cells into these anatomical areas will produce excellent results.
It is never a good idea to inject an excessively excessive amount of fat - the pressure exerted by the surrounding expanded tissues can compromise the survival of the fat cells (adipocytes). In other anatomical locations, such as the buttocks, such volume restrictions do not exist. Since the gluteal region contains a large amount of muscle mass, fairly large fat grafts can be safely placed in this area.
The maximum possible breast enlargement during one operation is limited to approximately 250 cm3
So what happens if patients request breast augmentation by more than one size? Any surgeon with extensive experience in breast augmentation will consider all possible options, but patients are usually offered a duplicate operation as an option.
Benefits of Breast Augmentation
Breast lipoaugmentation avoids the risks associated with alternative procedures such as tissue grafts and implants. There is no risk of developing an allergic reaction, since the transplants are part of the patient’s body.
Also, the main advantages of the technique include minimally invasive intervention and short rehabilitation.
Disadvantages of the method
Breast lipoaugmentation is limited to breast augmentation by one size and therefore cannot provide the large volumes that silicone implants can provide.
Between 20 and 25% of the grafted fat will likely be resorbed. This happens because fat, like living tissue, needs oxygen from the blood to survive and take root in a new place. Research is ongoing to determine which combination of techniques can reduce or prevent cell death. Researchers have recently done some very promising work with stem cells.
According to specialty website Modernmedicine.com, the unique advantages and disadvantages of breast lipoaugmentation make it especially suitable for use in conjunction with arthroplasty surgery. Rather than addressing the question of whether fat grafting or breast implants are appropriate, the authors of the article suggest that better results often result from a combination of the two methods.
The lipofilling technique is still one of the frequent topics of discussion at various congresses. There is ongoing professional debate about how much fat actually survives after lipoaugmentation, and there are ongoing concerns among patients about whether the surgery may make cancer more difficult to detect.
Is it necessary to do vacuum expansion before lipofilling of the breast?
Generally, vacuum expansion is not required before fat cell transfer. Preoperative vacuum expansion can be used for patients with limited "fat resources" and, most importantly, with dense skin. Considering that grafted fat does not tolerate pressure, it may be useful to expand the tissue before transplantation. The most popular way to do this is the so-called BRAVA external bra, which must be worn for several weeks before and after surgery. The extension can also optimize fat intake by several percent. So the use of an external expander can be useful, but these are rather exceptional cases.
Does lipofilling make it difficult to diagnose various diseases, including cancer?
Definitely not. A comprehensive review of the literature found that there is no conclusive evidence to date that fat grafts interfere with the detection of breast cancer. Women can take additional steps to ensure their safety and health by getting regular screenings like mammograms or MRIs. Fat cell transplantation is a plastic surgery with a high level of safety.
Is it possible to enlarge breasts by lipofilling by more than 1 size?
Yes, of course, but usually this effect can be achieved with a repeat operation. This means that during the first operation, plastic surgeons enlarge each breast to the maximum allowed (safe) amount, and a second operation is performed approximately three months later. This allows you to safely transfer up to 500 cm3 of fat.
Will breast augmentation with fat lead to superior aesthetic results?
The answer to this question is yes. Fat grafting surgeons have more control over the process of creating new breasts because they can target specific areas. They can make the necessary corrections in both the upper and lower poles of the breast.
Breast augmentation with lipofilling guarantees long-term results. In addition, this technique is an excellent way to correct the interthoracic space, the so-called cleavage.
Benefits of lipofilling
Adipose tissue contains a large number of stem cells, so the areas into which fat is pumped not only take on the necessary shape, but also acquire the necessary components that help smooth the skin, restore elasticity, and remove scars.
The lipofilling procedure is considered absolutely safe and is very popular because the skin looks very natural and patients tolerate it with ease.
- There is no allergic reaction due to the fact that rejuvenation occurs using the patient’s own tissues.
- There is a low probability of tissue rejection, along with the same artificial implants.
- After correction, the skin looks as natural and aesthetic as possible, due to the correction of two parts of the body at once.
- There is almost no trauma, and patients feel well and tolerate fat grafting.
- No anesthesia required.