Operations to change appearance are akin to the work of a sapper: even an experienced doctor can make a mistake. The numerous star “failures” that the tabloids are full of are the best proof of this. The dangerous aspect of any plastic manipulation is that the real effect cannot be seen immediately, and repeated operations are often required to correct the defects that appear.
Doctors rarely perform such operations for free, for example, for advertising purposes on the central channel. The actual delayed result is the only reason why it was possible to document the unpleasant aspects of plastic surgery
Non-star story
My friend rashly complained about stretch marks after giving birth. When asked what she plans to do about it, the answer was: “Nothing. I’m not a model, why do I need an absolutely perfect body? I love myself, carrying this baby, and my husband loves me like this.”
There are no ideal people; they often love these same imperfections in their loved ones as a unique feature. As you can see, even the excellent work of a surgeon will not bring you happiness if you yourself do not want to become happy and love the real you. And this problem cannot be treated with a scalpel. So go to the mirror right now, look into your eyes and feel how much you love yourself!
Back to the beginning of the article
Don't forget to like and rate the article!
Did you like the article? Subscribe to site updates via RSS, or follow on Twitter, VKontakte, Odnoklassniki, Facebook or Google Plus. And also receive new articles by E-Mail.
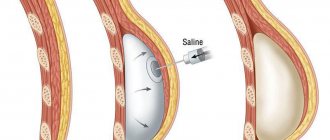
Postoperative asymmetry of the mammary glands
This problem can arise if breast implants are selected incorrectly. Breast asymmetry is also possible if it was observed in the patient before the operation, but for some reason was unnoticed by the surgeon. The specialist could install implants of the same size, so the asymmetry became even more pronounced. To eliminate such an error, the surgeon will need to perform an operation to replace one implant with a new one. This will help achieve the same breast size or at least minimize visible asymmetry.
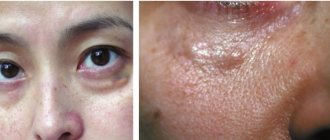
Eversion of the lower eyelid after blepharoplasty
One of the possible undesirable consequences of eyelid surgery is lower eyelid inversion. This may be caused by significant cutting of the skin and difficulty closing the eyes. Eversion of the lower eyelid can be corrected surgically, and after the operation the patient should not forget to perform an independent massage of the eye area to stretch the muscle tone.
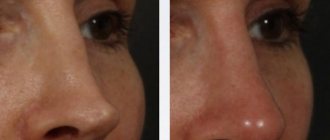
Nasal deformity after surgery
It is an extremely rare case that after rhinoplasty, with a pronounced degree of edema, deformation occurs, which subsequently persists even after the completion of the rehabilitation period. In this case, the plastic surgeon will be forced to perform a second operation under general anesthesia and reshape the nose. Of course, repeated operations with tissue modification are undesirable, so if it is possible to avoid repeated surgery, it is better to do so. But with significant changes in the nose, only a surgical method will help.
Implant contouring after cruroplasty
Cruroplasty will be successful if the plastic surgeon selects the correct implants. To do this, he will need to take into account all the individual parameters of the structure of the patient’s legs and legs as a whole, the characteristics of his figure and other proportions, and wishes for the future result.
If the implant is installed incorrectly or poorly selected, it may be contoured, a phenomenon in which its contours are clearly visualized. This can only be corrected through surgery.
Implant migration after gluteoplasty
Despite the fact that many plastic surgeons claim that such a complication is impossible, there is a lot of evidence that confirms the opposite. Even on the Internet, if you wish, you can find photographs and videos in which patients who have encountered such a problem show how the implant migrates inside the buttocks. Fortunately, even this error can be corrected. The surgeon will have to replace the implant or remove it completely.
Mammoplasty
What is this? Breast augmentation with implants.
Typical mistakes. Since the implant is a “stranger” for the body, it may be perceived inadequately. In an effort to get rid of the foreign body, the body builds up scar tissue around it, causing the breast to become rock-hard. In the language of professionals, this is called capsular contracture. Alas, even experienced surgeons can recall more than one similar case. Individual characteristics play a big role here, which even a professional cannot predict. The risk of contracture can be reduced by using implants with a textured surface.
Most “blunders” occur during the preoperative preparation process. Selecting an implant, choosing the right access, placing it so that no one would guess about it is a whole art. Alas, not all plastic surgeons can boast of artistic talent. So the lady gets unnaturally large breasts a la “star of the night air”.
How they are corrected. Almost always, the implant must be removed and then reinstalled. In case of encapsulation, you will have to wait at least six months, in other cases a couple of months is enough.
Mistake #6: Raised eyebrows
Sylvester Stallone is often the butt of jokes for having so much Botox on his face that he can barely move his lips. As it turns out, the actor is not the only fan of plastic surgery in his family. His mother, Jacqueline, also became addicted to modifications to her own face, already being a lady of advanced years.
Circular facelift, blepharoplasty, lip augmentation, correction of the shape of the nose, raising the eyebrow line, Botox injections - this is not the whole list of what Jacqueline did to herself. Today, the 97-year-old woman always looks surprised (or dissatisfied?) because of her perpetually raised eyebrows.
Mistakes during plastic surgery on the face
We believe that all errors that occur during reconstructive operations on the face mainly depend on improper planning of surgical interventions and errors in the surgical technique.
Planning errors mainly arise due to an insufficiently complete and detailed analysis of the patient’s defect. Of particular importance is a thorough analysis of the defect to determine the required amount of plastic material. For example, from the above photograph of a patient with an extensive defect in the middle part of the face (Fig. 458), it is clear that much more plastic material will be required to eliminate the defect compared to the size of the defect. This is explained by the fact that the organs that are to be restored must be two-layered. It is also important to take into account that after excision of visible scars, especially those located in depth, the size of the defect will increase even more. Ignoring these points prevents the correct and successful implementation of the reconstructive operation.
In addition, after excision of scars in the area of the defect, it is sometimes possible to bring out a completely preserved organ or part of it, which was drawn into the depths of the defect by scars (Fig. 459). After the displaced organ is installed in its place, the defect, on the contrary, decreases. Thus, we see the importance of correct analysis of the defect during facial plastic surgery.
It would be a mistake if a surgeon attempted to restore any organ on the face without the necessary support for it. Thus, in the absence of an alveolar process, the support for the restored lip should be a prosthesis. In case of an extensive facial defect, the nose can be restored when all the supporting parts on which the nose should rest (parts of the cheeks, upper lip, etc.) have been created.
The friendly work of a surgeon and an orthopedic dentist is important during plastic surgery on the face, since in some cases the restoration of facial organs (lips, chin, mandibular arch, etc.) requires the manufacture of appropriate prostheses and devices that ensure the correct design of the restored organs. A plan for a reconstructive operation that is not fully thought out, especially when it is multi-stage, often leaves the surgeon unable to complete the operation. In our clinic we observed such patients who were sent to complete the operation (Fig. 460).
Using a finger to reconstruct the nose should be considered a gross mistake [Tardie was the first to perform this operation in 1875].
Such an operation should at present be of historical interest only. However, back in the 30s, when surgeons already had at their disposal enough mastered methods of nose plastic surgery, in particular with the Filatov stem, we observed cases of using the index finger of the left hand to form a nose, and neither cosmetic nor functional success was achieved (Fig. 461, a, b).
In 2 such patients that we observed, the doctors, having removed only the nail before the operation, left the nail bed during finger transplantation, which led to the growth of a new nail (on the nose) after the finger was engrafted. There is nothing to say about the inadmissibility of such a quality as depriving a person of his index finger.
In one patient, when cutting out a flap from the forehead for the nose, the scalp was also included in the flap, so the entire nose was covered with thick hair (Fig. 462). One must also be careful when transplanting pedunculated skin flaps or when performing free skin transplants in boys, whose hair sometimes appears after 15-17 years. During operations, their skin should be taken only from those places where hair growth is not normally observed (the inner surface of the shoulder, forearm, thigh, interscapular area).
We consider it a mistake to cut out leather tape for the Filatov stem in the area of the elbow. The inability sometimes, due to limited skin mobility, to tighten the edges of the defect leads to wound healing by secondary intention and the formation of scars, causing contracture of the forearm.
Stems for restoring the nose or ear should not be cut out in places where there is a profuse subcutaneous fat layer. We also do not recommend introducing any supporting tissue (bone, cartilage, etc.) into the prepared stem in advance, which can significantly complicate all subsequent manipulations with the stem, since it is very difficult to calculate where the supporting tissue will lie after transferring the stem.
We have already noted that thanks to the use of antibiotics, the danger of postoperative inflammation and suppuration in the wound has been largely eliminated. However, observations show that technical errors can lead to partial or complete necrosis of the manufactured stem. For example, failure to observe the ratio between length and width (no more than 3:1) when cutting out the skin tape for the stem can lead to a sharp disruption in the nutrition of the stem and its necrosis. Necrosis can also be caused by an inappropriately large fat layer included in the stem, due to compression of the vessels and the development of stagnation in it. Necrosis of the so-called acute stem occurs if the length of the skin strip is twice as long as the width (1: 2).
When cutting out a skin tape, you must beware of excessive preparation at the ends of the incisions and tight tightening of the seams at the legs of the tape when sewing it into a stem. The legs of the tape should never be prepared beyond the end of the tape cuts, since the blood supply to the tape goes through the legs, which in these cases can be dramatically impaired. When rolling the leather tape into a stem, you must carefully check the color of the stem and its temperature. If the stem is very pale, then you should pay attention to the last seams on it: do they not tighten the tape too much? If necessary, they should be removed. If the manufactured stem has a cyanotic (stagnant) color and is cold to the touch, then you need to immediately make incisions on such a stem with a sharp scalpel, and sometimes remove one seam in the center of the stem.
When transferring a stem, it is necessary to ensure that the size of the area to which the stem is transferred is not less than the cross-sectional area of the stem, as this can lead to its death due to compression of the blood vessels. If the next day after the operation the stem is cold, and the transferred leg is clearly congested, it is necessary to make incisions on it and cover it with bags of ice (hypothermia), which leads to a decrease in blood flow, and, therefore, the stem can more easily cope with the difficult outflow of blood, from which he usually dies.
If possible, the stem sewn to the hand should be kept for no more than 3-4 weeks, since prolonged forced positioning of the hand can subsequently cause stiffness in the joints.
When transplanting tissue, we most often observe various complications depending on the incorrect technique. For example, when transplanting skin and fat, tissue trauma should be avoided. They should not be grabbed with tweezers when picking them up or when hemming them, but should be held on the stay sutures. Each grip with tweezers leads to crushing and disruption of the integrity of the capillary walls with subsequent death of the tissue in this place. To avoid catching the edges of the graft with tweezers while sewing it on, you should follow the rule: first stick the needle into the edge of the graft, and then into the edge of the receptive soil.
It is very important to follow the basic rule for all tissue transplants: the graft, after being taken, must be immediately transferred to a new bed. You cannot keep the transplant in various solutions (physiological, penicillin solution, rivanol, etc.) or wrapped in gauze until the bed is prepared. As a rule, the graft should be taken only after the receiving bed is completely prepared. The bed itself should, if possible, have a flat, smooth surface to ensure a good fit of the graft. During tissue transplantation, the use of adrenaline is unacceptable, since it constricts the blood vessels, which makes the initial gluing of the graft to the bed difficult. In addition, adrenaline promotes the formation of bruises when its effect wears off. It is also very important that the taken skin has the same thickness throughout, since this will ensure uniform pressure of the bandage and complete adherence to the receiving bed. The technique used by many surgeons, using a brush to grab, for example, the skin of the thigh in the form of a fold, should be considered incorrect. In these cases, the skin taken at the edges will always be thinner than in the center.
It is a mistake to take skin from the thigh, for example, for the tip of the nose or for the eyelid. The graft will stand out sharply in its color and thickness. In these cases, it is better to use skin from the upper surface of the chest or from the inner surface of the shoulder.
A few days after skin grafting, rejection of the superficial layers of the epidermis is often observed. It would be a grave mistake to consider this a sign of non-engraftment. As a rule, it always survives and therefore should not be removed. Only after 10-12 days can the issue of engraftment be finally resolved. We do not recommend using thin flaps (according to Thiersch) on the face, as they will stand out against the background of the surrounding skin for many years.
When transplanting fat under the skin of the face, which is usually done for cosmetic purposes, one must keep in mind that part of the fat is always subject to connective tissue degeneration. Therefore, it would be a mistake to make the fat graft the same size as the defect. The graft should always be 1/4-1/3 larger than the defect.
When cartilage is transplanted, suppuration is observed very rarely. However, if a purulent process occurs, the cartilage should not be removed immediately. It is necessary to make an incision, drain the pus and rinse the cavity with a solution of penicillin or another antibiotic. If after daily washing of the cavity for 5-6 days the discharge of pus does not stop, then the cartilage is removed.
Curvature of cartilage after transplantation under the skin of the nasal dorsum is often observed. This depends on the fact that the cartilage is taken from very young subjects and cut out at the site of the bend of the cartilaginous part of the rib along the connective tissue fibers.
It is advisable to use not very soft cartilage. The most durable cartilage is a slightly brownish color, not white.
Displacement of the cartilage transplanted under the skin of the nasal dorsum may depend on asymmetrical skin detachment and improper application of the dressing. The bandage should be removed no later than 6-7 days after the operation in order to be able to, until the graft has grown firmly, simply press the finger on the skin to put it in the correct position. Displacement of the cartilage often occurs because its upper end is not inserted under the periosteum of the nasal bones and therefore becomes mobile.
The cartilage inserted under the skin of the back of the nose should not be very large, so as not to cause pressure sores on the skin.
We consider the introduction of cartilage into the Filatov stem in advance, before the creation of any organ (nose, ear, etc.), as this will sharply limit the surgeon in his manipulations due to the difficulty of foreseeing in advance how the cartilage will lie in the newly created organ .
In the corresponding section, we have already indicated that when taking costal cartilage, damage to the pleura is possible. The latter circumstance can be avoided if, when cutting out cartilage, the knife blade is held not perpendicular, but obliquely to the middle of the rib. In addition, pleural rupture often occurs at the last moment of cartilage harvesting, when the surgeon, without carefully freeing the graft, tries to tear it out from the surrounding tissue. In these cases, the pleura is ruptured because it is pulled behind the perichondrium, which the surgeon is trying to tear off.
To eliminate the possibility of compression of the lung by air, sutures should be quickly placed on the intercostal muscles.
When transplanting a bone graft from a rib or ilium, complications are possible, which we have already written about (tissue transplantation). You just need to add that the graft should always be several centimeters (5-7) longer than the defect so that it fits firmly on the ends of the fragments. If the resulting graft turns out to be insufficient in size, it is better to replace it with another one.
When transplanting bone into a defect in the lower jaw, it is especially important to prepare in advance a fixation device that would not require prolonged manipulation in the mouth after transplantation, as this can lead to displacement of the graft.
The last thing we would like to dwell on is errors in the treatment of wounds caused by improper restoration of damaged organs.
These errors partly depend on the doctors’ lack of familiarity with the principles of facial reconstructive surgery, partly on insufficient attention, especially during the initial treatment of the wound, which can sometimes be explained by a certain haste in the work. As an example, we can cite a case (Fig. 463) when the torn cover of the face and head was sewn in the wrong place, as a result of which the torn palpebral fissure ended up on the left cheek.
For another wounded man at one of the medical stations on the front line, when providing first aid, the torn nose was sewn with the nasal openings not down, but to the left side (Fig. 464).
It is difficult to list all the mistakes that are possible during facial reconstruction operations. However, there is no doubt that with the surgeon’s attentive and careful approach to the patient, with a carefully drawn up sequential operation plan and a detailed analysis of the defect, many mistakes can be avoided. Of course, the technical capabilities of the surgeon are also of great importance for the success of the operation. A doctor involved in facial reconstructive surgery must remember that every mistake at some stage of plastic surgery entails failure, and every failure, in turn, extremely traumatizes the psyche of the patient, who is already often depressed by his disfigurement.
Elsa Patton
The star of the reality show "Housewives of Miami" Elsa is called the sister of "Catwoman". Well, they have a lot in common: a huge fortune, no wrinkles and a love of plastic surgery. There are no photographs of the star before plastic surgery, since she went under the surgeon’s knife in her youth. But on the Internet there is a photo of her daughter, Marisol Patton, who seems to be going to follow in her mother’s footsteps.
Elsa Patton lived to be 84 years old and is remembered by the world for her smile. One of the operations turned out to be too unsuccessful: huge implants were inserted into the American woman’s lips. After this, they began to talk about the wealthy lady as if her smile was carved with a knife. Patton is an example of the fact that in the pursuit of excessive rejuvenation, the main thing is to stop in time.
Complications after otoplasty and contraindications
Correction of the ears is one of the safest operations in plastic surgery. However, due to unprofessional surgical intervention, some postoperative complications may occur:
- formation of hematomas and edema, which can lead to necrosis of cartilage tissue;
- allergic reactions of the body to suture material;
- development of inflammatory and purulent processes in the area of surgical intervention;
- atrophy of tissue in the surgical area due to impregnation with antiseptic agents;
- the formation of scars (this problem can arise both as a result of inaccurate suturing, and as a result of physiological predisposition);
- removal of the extended ear;
- distortion of the ears.
Surgeons' mistakes during otoplasty
Otoplasty is contraindicated in patients with the following clinical abnormalities:
- exacerbation of infectious and sexually transmitted diseases;
- disorders of the thyroid gland;
- development of cancer;
- diabetes;
- chronic diseases (during exacerbation).
Mistake #2: a sunken nose
Another “record holder” for plastic surgery is Michael Jackson. The king of pop not only completely redid his face, but also changed his skin color and hair structure. However, it was the wide nose that always seemed to be the main problem for the singer, so he underwent the most merciless changes.
Michael underwent several operations, but in the end the world star’s nose became very small, almost lost its cartilage tissue and literally “failed,” which is why Jackson often hid it behind a scarf, hiding from the paparazzi.